
In May, I had the privilege of chairing the World Conference Forum 2026 Hospital Patient Flow Management Conference in San Diego, CA. It was two days of conversations with patient flow leaders from across the country, and covered everything from ED boarding to command center design.
Throughout the day, on key theme emerged: it’s not about the number of resources you have in your system, it’s how you strategically leverage what you have to drive better flow. Here are three examples from the day that stuck with me.
How Stanford Health Care Redesigned Its Emergency Department Without Adding a Single Room
The instinct when an ED gets crowded is to ask for more rooms. Dr. Sam Shen from Stanford Health Care spent his session explaining why that’s usually the wrong question.
Stanford’s ED sees over 112,000 patients a year. ESI 1-2 (their sickest patients) climbed from 25% to 31% of their volume over four years. That squeeze pushed lower-acuity patients into longer waits and higher Left Without Being Seen (LWBS) risk.

Dr. Shen segmented his team’s initiatives across three areas: entrance and triage, within the ED, and disposition. The physical space tactics alone sparked the most conversation in the room:
- Implementing Vertical Flow Zones: Stanford carved a section of the ED lobby into a dedicated vertical flow area for lower-acuity patients. Patients are seen in chairs providing a low-cost solution to over crowding, decreasing length of stay for emergency severity index (ESI) 3 patients.
- Converting the Transportation Lounge: Stanford converted an existing transportation lounge into eight new treatment spaces. No new construction required.
- Leasing an Overflow Facility: Stanford leases 24 beds in a nearby facility to create additional capacity during peak demand.
In addition, the Stanford ED team built a virtual fast track program that has treated more than 9,300 patients since December 2020. The 72-hour return rate came in at 3.5%, compared to 3.9% for traditional ED patients, and wait times dropped by 49.2%.
The through line in Dr. Shen’s work that patient flow leaders must always keep in mind: how can we optimize the resources that we already have by triaging properly and maximizing the utility of existing physical space?
The Discharge Barriers Extending Length of Stay

Some patients are ready for discharge long before discharge is ready for them. Dr. Carissa Tyo from UI Health presented on the barriers that extend length of stay far past clinical necessity.
For patients with extended length of stay (LOS), the top barriers were pending guardianship (35%), financial and insurance barriers (26%), and complex family dynamics (18%). For patients with LOS over 30 days, pending guardianship climbed to 42%.
“Development of a [transportation] network surrounding your hospital and recruiting allies from your region will prove exceptionally beneficial in your management of complex cases.”
– Dr. Carissa Tyo, UI Health
Dr. Tyo’s team designed their response to address each barrier at its source:
- A physician advisor program with direct Epic Secure Chat access
- Multidisciplinary rounds scripting for care planning
- Payer direct access to medical records
- Early network referrals for post-acute placement
But the multimodal response only works, she argued, if someone owns it; Dr. Tyo said that every health system needs a focused, skilled internal subject matter expert with a dedicated complex care service line. Or, as she put it, a “Dennis.” Your system’s “Dennis” should be someone who can handle repatriation, knows every embassy contact, and every medical transport vendor for international returns. This is also someone who manages guardianship cases start to finish and shows up for the frequent fliers with behavioral health challenges, substance use barriers, or criminal history that limits placement options.
Someone who manages guardianship cases start to finish and shows up for the frequent fliers with behavioral health challenges, substance use barriers, or criminal history that limits placement options. Complexity at this level requires a specialist. It cannot, and should not, live on the desk of an already-overloaded case manager.
The UCLA Health Command Center Approach That Improved Transfer Completion
Scott Jahnke, Senior Director of Operations at UCLA Health’s Patient Flow Command Center challenged most of the command center & patient flow discussions I’ve been in for the last two years. Jahnke argued that if your system only activates when things go bad, you’ve already lost. You’re reacting to a system in failure instead of a system learning from itself. His charge to the room was simple: shift your existing system from reactive to learning.
“Flow isn’t just about movement—it’s about meaning. When your system starts learning, every referral, every bed, and every decision starts working together.”
– Scott Jahnke, UCLA Health
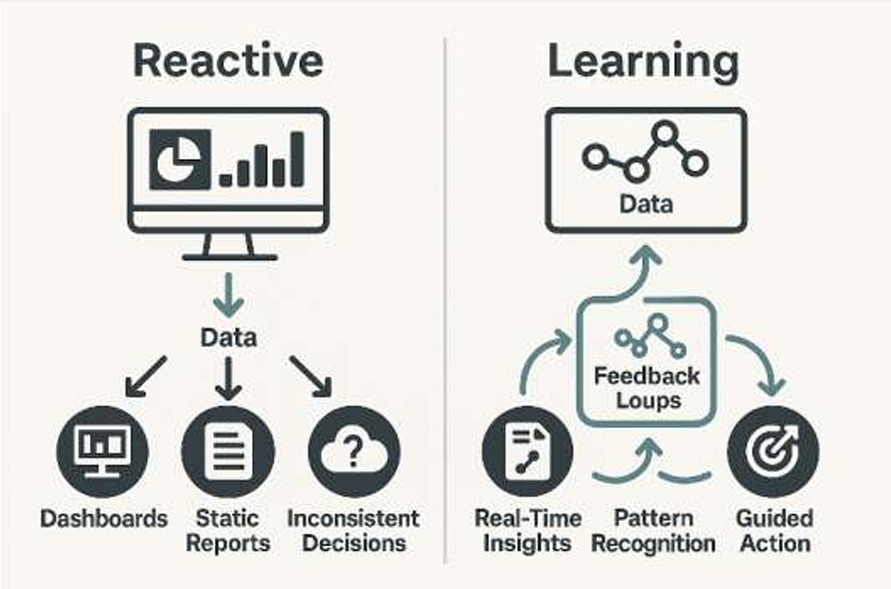
From Reactive Escalation Centers to Adaptive Learning Systems
In practice, that shift comes down to how a system repurposes the information it already has. Reactive systems have dashboards that react in the moment to spikes and drop-offs. Learning systems have feedback loops that develop proactive measures to anticipate future problems.
Unlike reactive systems, learning systems use Statistical Process Control (SPC) to distinguish between common cause variation (noise, normal fluctuation) and special cause variation.
At UCLA Health, Jahnke’s team used SPC charts to examine length of stay variation for transferred patients. They identified where variation was systemic and where it was an outlier. Analyzing this data helped his team stop reacting to every bump — instead, they were able to start asking why patterns existed and how to shift them.
After Jahnke’s team shifted the way they utilized their existing data, transfer completion from referring facilities rose from 40% to over 50%. Lost referrals dropped from one in five to fewer than one in eight. In the first two months, commercial transfers ran at 114% of baseline.
The data to improve your system is already there. Jahnke’s broader argument was about building the culture to actually use it. Stop counting how many times your command center intervenes, or how many metrics are sitting “in the red” and start asking whether the people doing the work can spot a problem and fix it. That’s where the real optimization happens.
The Strategic Shift Patient Flow Leaders Are Making in 2026
What really stuck with me from this conference was how the best systems think about how patient flow fits within the system itself. Instead of one singular tactic or takeaway, I was really struck by how presenters were rethinking and leveraging resources in every way possible. Stanford didn’t need to build more rooms for it’s crowded ED, it just needed to repurpose the space they already had. When UI Health needed to speed LOS, they realized a multi-modal approach owned by a specialist worked better than adding more case managers. UCLA Health changed how and when they looked at the data; they didn’t build a bigger and better dashboard.
These organizations tackled critical patient flow barriers by leveraging a smarter relationship with resources, data, and the people already inside their organizations.
Ultimately, I can’t help thinking about how the same principle applies to patient transportation. Health systems getting the best results treat transportation as a designed system. They measure it seriously, escalate intelligently to solve root causes, and give their teams the tools and context to actually improve over time. These teams also recognize transportation insights can be applied to more than just if a ride showed up on time, and actively use this data to discover further patient flow bottlenecks.
Your transportation strategy (and corresponding platform) is a key existing resource to accelerate flow at your organization; if you’re not currently leveraging that data, now is the time to start.

Lindsay (Tsai) Tamchin is the Chief Revenue Officer at Roundtrip. She leads all revenue-generating activities at the company including marketing, business development, sales, and account management. Since joining in 2017, she has led the efforts to secure 85+ contracts across the country. She attended the University of Pennsylvania where she received her BSE in Materials Science Engineering and a minor in Engineering Entrepreneurship.