
The Rural Health Transformation Program (RHTP) represents one of the most significant federal investments in emergency and community-based care in US history. Anchored in a focus to expand equal access to care to Americans in rural communities, these federal funds also work to offset the significant Medicaid cuts passed in the same federal budget law that created the RHTP.
As states start to strategize on where to use their funds, their prioritization could have cascading impacts on the EMS agencies who serve them. Dispatch centralization, 911 diversion, workforce development, and direct patient care all face disruption – for better and for worse.
States building their rural health programs need a partner who understands emergency care on the ground, and EMS agencies that engage now are positioned to strategically drive impact. We break down everything your agency needs to know about the RHTP, from funding timelines to how to position your agency for a seat at the table.
What Is the Rural Health Transformation Program?
The Rural Health Transformation Program (RHTP) is a federal initiative through the Department of Health and Human Services designed to drive lasting structural change in how states deliver emergency and community-based care. Authorized by the One Big Beautiful Bill Act and administered by CMS, the RHTP provided $50 billion in funding across five fiscal years beginning in 2026. All 50 states were eligible to apply, and funded projects had to target measurable improvements across areas like chronic disease management, workforce development, and emergency care delivery.
Specific programs vary by state, but for EMS agencies developing proposals, every project should map clearly to at least one of these CMS objectives.
- Make Rural America Healthy Again: Support rural health innovations and access points that promote preventive health and address the root causes of disease.
- Sustainable Access: Help rural providers become long-term access points for care by improving efficiency and sustainability.
- Workforce Development: Attract and retain a high-skilled healthcare workforce by strengthening recruitment and retention in rural communities.
- Innovative Care Models: Spark the growth of care models that improve health outcomes, coordinate care, and promote flexible care arrangements.
- Tech Innovation: Foster the use of innovative technologies that promote efficient care delivery, data security, and access to digital health tools.
Regardless of how states allocate their funds, programs must be built to sustain themselves long after the funding ends. Two key examples are already taking shape: states are centralizing EMS dispatch and redirecting lower-acuity 911 calls to more appropriate care settings. That includes addressing the barriers that keep patients from reaching care in the first place, transportation among them.
Cultivating EMS and State Government Relationships Before the RHTP Funding Arrives
The states making the fastest progress on RHTP implementation share a common advantage: strong relationships between EMS leadership and their state Departments of Health. When these relationships are already in place, funding approval moves faster and project implementation starts stronger.
One Rural Health Transformation Program panel at ESO Wave 2026, moderated by Asbel Montes, co-founder of Solutions Group Services, offers a clear case study. In the panel, Hawai’i state EMS Chief Garrett Hall described how Hawai’i is consolidating EMS dispatch services under the state’s Department of Health. The project attempts to coordinate EMS across a landscape where different islands operate under entirely different service models, from county-run systems to fire department partnerships to state-contracted providers. Chief Hall explained, the “progress made so far has reflected years of coordination between state agencies, emergency responders, and hospitals working to strengthen Hawai’i’s emergency medical system.”
“Progress made so far has reflected years of coordination between state agencies, emergency responders, and hospitals working to strengthen Hawai’i’s emergency medical system.”
– Chief Garrett Hall, Hawai’i state EMS Chief
Minnesota offers another example of how prior groundwork translates directly into RHTP momentum. Dylan Ferguson, Director of Minnesota Office of EMS, describes his state’s approach as deliberately building on an existing Treatment in Place (TIP) model that EMS agencies had already established relationships around. Rather than starting from scratch, Minnesota identified that existing program in its RHTP application to CMS, aligning it with sample programming in the Notice of Funding Opportunity and tying it across multiple CMS objectives and state strategic initiatives.
Clear reporting against success metrics was a critical component of how Minnesota measured the program’s impact. “We really want[ed] this as streamlined as possible and are working to leverage already existing sources of data as much as possible for participating agencies,” says Ferguson. The result was a competitive RFP process through which rural agencies can participate in a TIP program administered by the Office of EMS, with reimbursement available for clinically meaningful care provided without transportation.
The speed both states achieved after funding arrived was a direct result of the relationships they had cultivated long before the application process began. EMS agencies that prioritize those relationships now will be the ones best positioned to shape how RHTP dollars flow in their states.
Can Your Operations Scale to Support RHTP Initiatives?
As EMS agencies adjust to support statewide RHTP initiatives, your dispatchers and health system partners will all need to operate from the same data. A ride booking platform that centralizes all ride requests and automates notifications keeps everyone on the same page.
Learn how Roundtrip can help your operation scale.
How RHT Programs Are Tackling 911 Overutilization
Alongside the effort to centralize dispatch, another focus of some RHTP-funded programs is to identify and redirect lower-acuity 911 calls. According to a 2024 ESO research study across the US, an estimated 92% of calls to 911 are not truly time-sensitive emergencies. Perhaps counterintuitively, the highest utilizers of EMS services, those who call six or more times per year, are actually the lowest-acuity patients.
This creates a clear opportunity. Diverting the highest-utilizing, lowest-acuity patients to the resources they actually need can have wide-ranging benefits:
- Patient outcomes: Patients can establish ongoing relationships with providers who manage chronic conditions holistically, rather than cycling through emergency departments.
- EMS capacity: Resources are preserved for the 8% of 911 calls that are truly time-sensitive emergencies.
- Transportation access: Patients who are diverted can be connected to reliable non-emergency transportation that consistently gets them to the level of care they need
- System-wide savings: The entire healthcare system benefits fiscally by driving better outcomes at a lower cost.
Transportation Is Central to Rural Health Transformation Program’s Success
The goal of the Rural Health Transformation Program is to get every patient to the right level of care. In rural communities, where access to public transit is limited and personal vehicle access can be unreliable, transportation is frequently the barrier standing between the patient and the care they need.
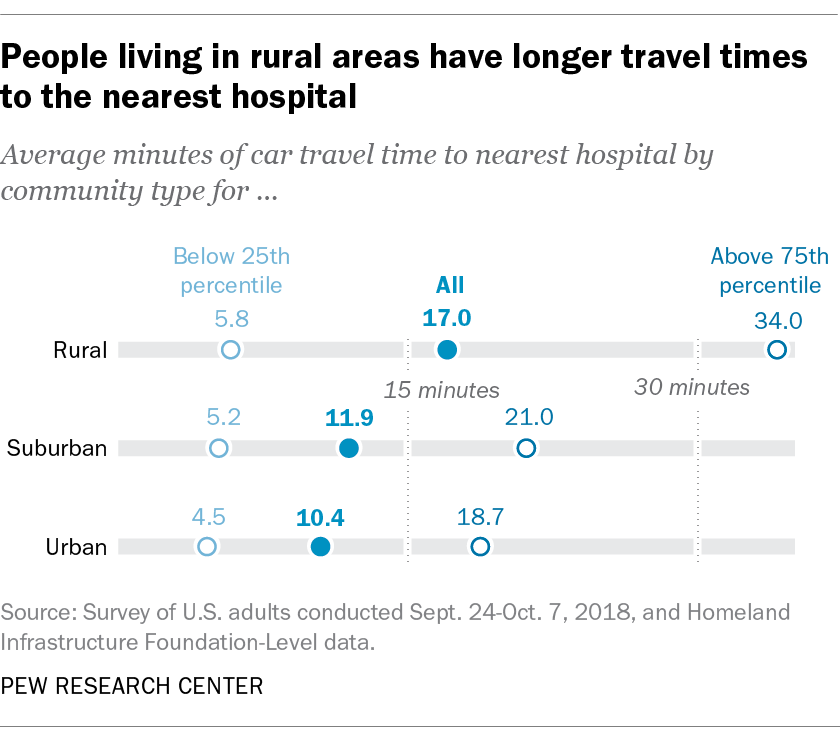
5.8 million Americans delayed medical care because they did not have transportation in 2017 alone. Nearly a decade later, the problem remains — and it falls hardest on the patients living furthest from care. Unlike their urban counterparts who can rely on public transit or shorter travel times, rural patients travel 2 to 3 times farther to obtain healthcare, with far fewer alternatives when their primary transportation method falls through.
Improving rural health outcomes has been a focus for some time, with renewed urgency this past year as states submitted their proposed budget allocation plans. While we budget plans have been approved for funding allocation, there is still time to influence how those funds are deployed. EMS agencies that make improving rural transportation access a visible part of their proposals will be better positioned to shape how state-funding is distributed.
CMS’s ET3 Program: An Imperfect Blueprint for the Rural Health Transformation Program
The Emergency Triage, Treat, and Transport (ET3) program was a Centers for Medicare & Medicaid Services (CMS) pilot launched in 2020 that gave EMS agencies a new option: rather than defaulting to an ED transport, agencies could treat patients in place or connect them with alternative care.
Over its three-year run, ET3 showed an average Net Savings to Medicare (NSM) of over $500 per beneficiary “when a patient was treated-in-place instead of taking an ambulance ride to the hospital emergency room”. However, due to CMS’s regulatory structure, ET3 could only apply to traditional Medicare fee-for-service beneficiaries, which significantly limited its reach. That limited reach reduced provider willingness to participate, and CMS wound down the ET3 program in 2023.
What Makes Rural Health Transformation Different This Time?
ET3 proved the model works, but structural limitations kept it from scaling. The Rural Health Transformation Program addresses those gaps directly, bringing several advantages that ET3 lacked:
- Implementation funding, not operational dependency: RHTP provides funds for implementation, but specifically bars that funding from ongoing operations. These programs must eventually be self-sustaining, which builds in a discipline that pilots like ET3 didn’t require.
- Medicaid inclusion: By involving individual state Departments of Health, Medicaid populations can now be covered under 911 diversion initiatives — a critical expansion beyond the FFS-only limitations of ET3.
- A data foundation for the future: The systematic collection of key performance metrics across all RHTP initiatives gives stakeholders the evidence base to continue the conversation. Over time, that foundation could drive adoption into the commercial payer space.
How EMS Leaders Can Engage With Rural Health Transformation
The Rural Health Transformation Program is a once-in-a-generation opportunity to change healthcare, and the EMS industry needs a seat at the table for these initiatives to succeed. Here are a few specific, actionable steps EMS leaders can take today:
- Find your state’s open grant opportunities: Federal funding has been awarded to all 50 states, but many states are still distributing RHTP funds to local organizations through open grant programs. Find the right person in your state’s Department of Health and put a proposal in front of them.
- Register as a vendor with your state’s procurement system: Most states require your agency to be properly registered in order to apply for and accept funding. Get ahead of this hurdle by confirming your status in your state now.
- Position transportation as part of your RHTP strategy: The agencies best positioned to demonstrate measurable outcomes under RHTP are the ones treating transportation as a core component of care delivery, not an operational afterthought.
- Get involved in EMS associations and trade groups: A unified industry voice across your state carries far more weight than individual organizations advocating in isolation.
First-year projects are already funded and underway. The groundwork being laid right now will determine what rural emergency care looks like for the next decade. The EMS agencies that build relationships with state Departments of Health and demonstrate measurable outcomes will be positioned not just to benefit from RHTP funding, but to shape whether EMS earns a permanent seat at the table for statewide rural health planning in the years to come.

Sze Hui, CSPO has spent over 8 years in the healthcare industry, leading efforts to optimize workflows and eliminate copy/paste through data interoperability and integrations. As a Solutions Architect, Sze guides health systems through the technical implementation process, bringing data flow and business process together in a cohesive and seamless way.